How We Work

Enhancing, not duplicating
We’re not trying to reinvent the wheel, and we’re not starting from scratch. There are already many efforts around the world to strengthen health data. Our role is to build upon existing efforts by establishing a network of technical working groups that will address specific technical issues and identify and fill technical gaps.
The working groups develop standards, indicators and other tools that help countries to collect, analyse and use good health data. At the same time, we work to make sure everyone is pulling in the same direction, to support the health plans and priorities that countries set.
The working groups are time-limited groups of technical experts from partners, countries, academia and civil society that are brought together to work collectively on specific deliverables of the Collaborative’s work plan. This could entail the development and harmonization of standards and tools to strengthen country health information systems and capacities.
Our governance structure
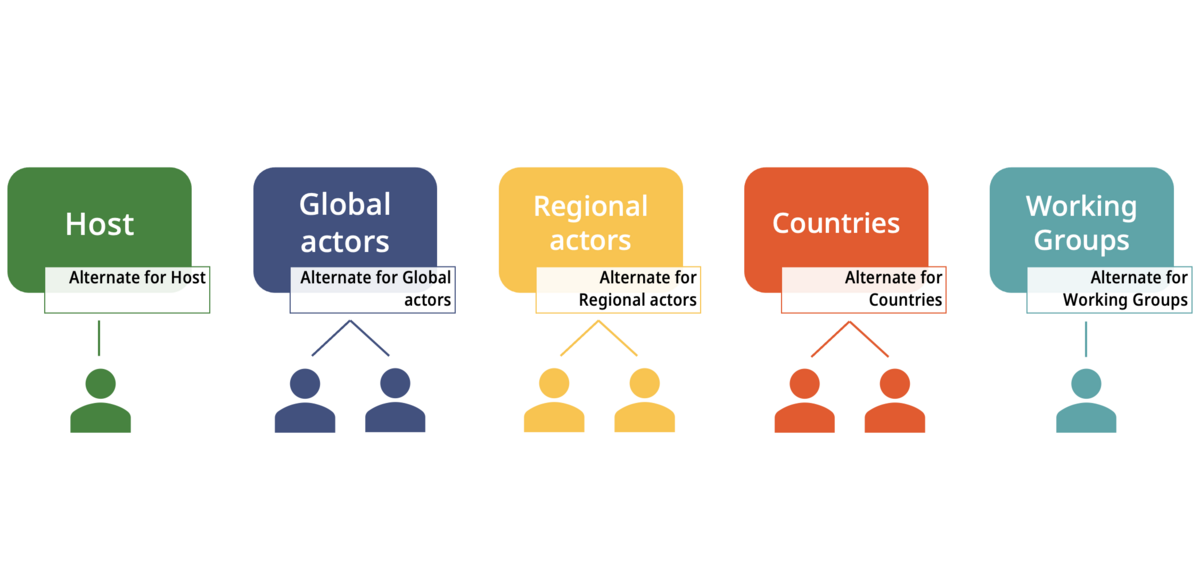
The HDC membership is diverse and, depending on the nature of their contributions, members are organised in seven constituencies: i) Countries, ii) Bilateral Donors, Philanthropic Institutions and Regional Funding Entities, iii) Civil Society, iv) Private Sector, v) Multilateral and Intergovernmental Organisations, vi) Research, Academia and Technical Networks and vii) Global Health Initiatives.
This increases diversity of view-points, technical and financial inputs, geographical perspectives, contexts and gender. To provide strategic guidance and direction to this rich membership composition, HDC governance is structured around a Board of Members, with a mandate to:
- Provide oversight and offer strategic direction to the HDC (i.e., define objectives and scope of work through quarterly meetings);
- Review and approve HDC work plan and budget;
- Assess progress and needed course corrections;
- Identify, assess, and mitigate the key risks that could hamper HDC objectives; and
- Guide strategic allocation of resources (technical, financial and political) within the HDC
The Terms of Reference for the HDC Board, with details on each type of Board Member, duration of appointments, and else can be found here. This structure allows the HDC to collectively leverage expertise, tools, technologies and partnerships to achieve its objectives and serve countries’ data needs.
HDC Board composition 2024-2025
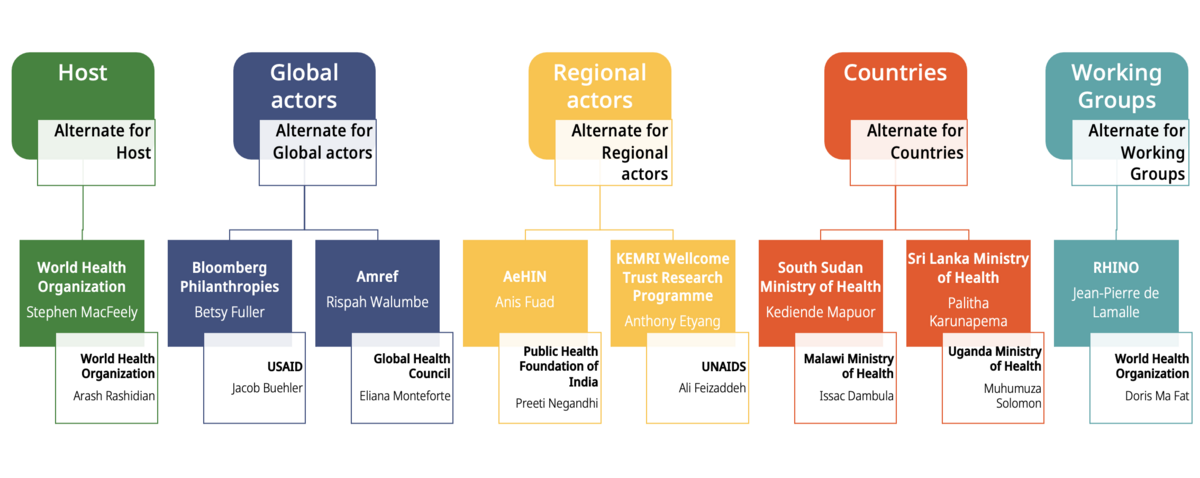
Meet your Board
Members

Asia e-Health Network (AeHIN)
Indonesia

KEMRI-Wellcome Trust Research Programme
Kenya
Prof Anthony Etyang has a background in Internal Medicine and Epidemiology and is the Head of Epidemiology and Demography at the KEMRI-Wellcome Trust Research Programme in Kenya. He is part of a team that oversees the Kilifi Health and Demographic Surveillance System, a large population level surveillance system that has been running for over 20 years. His research work focusses on improving the generation and availability of locally relevant data for addressing a variety of infectious and non-communicable diseases in Kenya and other low-income countries.

Bloomberg Philanthropies
United States

European Agency for Development and Health
Co-chair, Routine Health Information Systems Working Group, HDC
Brussels, Belgium
Dr. Jean Pierre de Lamalle is a senior expert in public health and health information systems, co-founder, co-owner and board member of AEDES (European Agency for Development and Health), a public health organization based in Brussels. He has worked in many countries to support HIS and has contributed to the development of books and training programmes on HIS. He is Chairman of the Board and President of RHINO (Routine Health Information Network Organization), USA, and is actively engaged in Health Data Collaborative, HDC (co-chairing the HDC RHIS working group) and since 2024 member of the Board of Directors.

Ministry of Health
South Sudan

Ministry of Health
Sri Lanka

Senior Health Policy Advisor
AMREF
Kenya
Dr Rispah Walumbe is a Global health specialist with a decade of experience in advocacy and healthcare policy at a national, regional, and global level. Her focus and training are in Healthcare Policy and Financing, and currently practices as the Senior Health Policy Advisor at AMREF Health Africa where she leads the UHC Delivery Lab a regional technical hub that serves as a collaborative knowledge platform to advance progress towards UHC in Africa. She also sits on the Advisory Group for the Civil Society Engagement Mechanism for UHC2030 and leads the coordination for the informal Ministerial Caucus, the Africa Health Leaders Policy Forum.

Director of Data and Analytics
World Health Organization
Geneva, Switzerland
Steve MacFeely is the Director of Data and Analytics at the World Health Organization and Adjunct Professor at the Centre for Policy Studies at University College Cork in Ireland. Steve is the co-chair of the Committee of the Chief Statisticians of the UN System (CCS-UN) and is an elected member of the International Statistics Institute. He co-led the Data Strategy of the Secretary-General for Action by Everyone, Everywhere 2020-2022, and was a lead author of the 2020 System-wide Roadmap for Innovating UN Data and Statistics. Before joining WHO, Steve was the Head of Statistics and Information at UNCTAD and was also the Deputy Director-General at the Central Statistics Office (CSO) in Ireland.
Alternates

Head, Strengthening National Capacities and Dissemination
UNAIDS
Nairobi, Kenya
Ali Feizzadeh currently heads the UNAIDS team on Strengthening Capacities and Dissemination, Data for Impact. He is currently based in Nairobi, Kenya and in the past 17 years has worked in South Africa, Papua New Guinea and Iran Country Offices as well as at the Regional Support Team for Middle East and North Africa, based in Cairo. Before joining UNAIDS, he worked with several UN agencies, research Institutes, the Ministry of Health, and Social Welfare Organization, all in Iran.

Director of Science, Information, and Dissemination
WHO Regional Office for the Eastern Mediterranean
Cairo, Egypt
Prof Arash Rashidian (MD, PhD) is the Director of Science, Information, and Dissemination in the WHO Regional Office for the Eastern Mediterranean and has led WHO regional agenda in areas of evidence-informed policymaking, health information systems, digital health, research promotion and governance and knowledge sharing since 2015. He has an established career in health policy research and health system development, with extensive experience in several countries. He is the Vice-Chair of WHO’s Guideline Review Committee. During the COVID-19 pandemic, he led the Research and Knowledge Management Pillar of the WHO Response Management team in the Region.

World Health Organisation
Co-chair, Civil Registration and Vital Statistics Working Group, HDC
Geneva, Switzerland
Doris Ma Fat’s responsibilities over the past 24 years have been focusing on cause-of-death statistics. As a statistician, she ensures the WHO Mortality Data base currently hosted in the Department of Data and Analytics is regularly updated with data from Member States. She also makes the data available to researchers and undertakes analyses pertaining to the mortality component of the burden of disease analyses. In addition, she develops electronic tools for analysing causes of deaths and supports countries in improving the quality of their mortality data.

Eliana Monteforte
Director for Special Projects
Global Health Council (GHC)
United States
Eliana Monteforte is the Director for Special Projects at Global Health Council (GHC) where she leads advocacy efforts focused on improving community and civil society engagement and advocating for key health equity issues globally. For over 15 years, Eliana has worked with civil society organizations (CSOs) and governments around the world to build strong health programs, products, and services that are responsive to populations’ needs, particularly those most vulnerable and marginalized. For many years, Eliana also worked with the Ministries of Health in Angola and Honduras to strengthen their health information systems (HIS) and develop regional and district-level health plans and budgets as well as health watch monitoring frameworks to monitor access and quality of health services.

Ministry of Health
Malawi

Senior Advisor
USAID’s Office of HIV/AIDS
United States
Jacob Buehler is a Senior Advisor at USAID’s Office of HIV/AIDS advancing the appropriate use of data and digital health. He has 15 years of experience supporting the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) program, focused on health information systems implementation; HIV monitoring and evaluation; health systems capacity; and IT project management. He has supported activities in a range of countries including Ethiopia, Lesotho, South Africa, Tanzania, Uganda, Vietnam, and Zambia. Prior to his work in global health, Jacob was a project manager in the online education sector and worked in the tech sector in San Francisco during the early dot-com era. He received a master’s degree in health policy from Johns Hopkins University and earned his undergraduate degree from Wesleyan University.

Indian Institute of Public Health
Delhi, India
Preeti Negandhi has medical and public health qualifications. As a senior faculty at the Indian Institute of Public Health - Delhi, an academic Institute of the Public Health Foundation of India (PHFI), she teaches post graduate students across PHFI’s on-campus and eLearning programs. She also leads several capacity building initiatives at the Institute, in epidemiology, research methodology and routine health information systems. As a researcher, her areas of work include program evaluation, maternal new-born and child health, health information systems, health systems strengthening. She was actively involved in the SCORE assessment for SEAR countries (2018-19) and leads the capacity building portfolio for RHIS – Basic Concepts and Practice at PHFI since 2016.

Ministry of Health
Uganda
Solomon Muhumuza is a Digital Health Specialist with over 7 years of supporting national scale of digital health interventions including Electronic Medical Records systems (EMRs). Solomon has supported the set-up of critical digital health governance structures at the national level and coordinated the development of key governance and security frameworks like the Uganda Health Information and Digital Health Strategic Plan 2020/21-2024/25. Solomon holds a Master's Degree in Computer Science from Robert Gordon University, Scotland and currently, Solomon is the secretary for the Health Information Innovation and Research Technical Working Group at the Ministry of Health.
